Hip resurfacing removes less bone than a total hip replacement and is often promoted to those who wish to resume running, tennis, and other high-impact sports after surgery. However, resurfacings represent less than 1% of hip replacements annually, and few surgeons perform the procedure. In addition, most resurfacings use metal-on-metal constructs that produce potentially harmful metal debris. The best candidates for hip resurfacing are younger than 60, have larger frames and strong, healthy bones. Resurfacing is not recommended for patients who are older, female, and smaller-framed. Recently, ceramic-on-polyethylene and ceramic-on-ceramic constructs have appeared, with the goal of addressing both metal debris and demographic restrictions.
I’m not a medical professional, and I'm not offering medical advice. You should consult with a physician or other qualified medical professional for diagnosis, treatment, and advice. The content on this site is for informational purposes only.
There are two main types of hip replacement surgeries: total hip replacements and hip resurfacings. The vast majority of hip replacements in the U.S. and worldwide are total hip replacements. In this post, I’ll briefly explain the key differences in the two procedures and then discuss hip resurfacing in more detail.
As an aside, I’ll mention that a way to regenerate cartilage always seems to be right around the corner (Stanford 2020; Duke 2020; Johns Hopkins; Mayo Clinic 2023; Northwestern 2024; Stanford 2025). Similarly, an absorbable implant designed to mimic cartilage is currently in Phase I trials (ReNew). Neither of these technologies address other symptoms of hip osteoarthritis (OA), such as osteophytes and labrum damage, and so might not be sufficient to treat advanced hip OA, even if they ultimately repair cartilage damage.
In a total hip replacement, the femoral neck and head are removed and a metal stem is inserted into the femur. An artificial ball (also called a “head” or “bearing”) is placed on top of the stem. A metal cup is inserted on the acetabular side. Typically, a liner is inserted into the cup to interface with the ball. Thus, there are four main components to a total hip replacement:
A total hip replacement is also known as a “total hip arthroplasty” (THA). Here’s what the components look like:
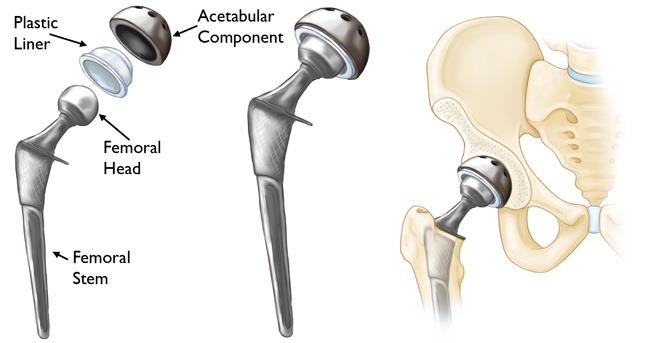
(Image from OrthoInfo, the website of the American Academy of Orthopedic Surgeons.)
In a hip resurfacing — also called hip resurfacing arthroplasty (HRA) — the femoral head and neck are preserved. The head of the femur is trimmed and capped. The cap has a stem that inserts through the head into the neck. As with a total replacement, a cup is inserted on the acetabular (socket) side. Sometimes a liner is inserted in the cup to interface with the capped head. A hip resurfacing may therefore contain two or three components:
Here’s what each looks like on X-ray.
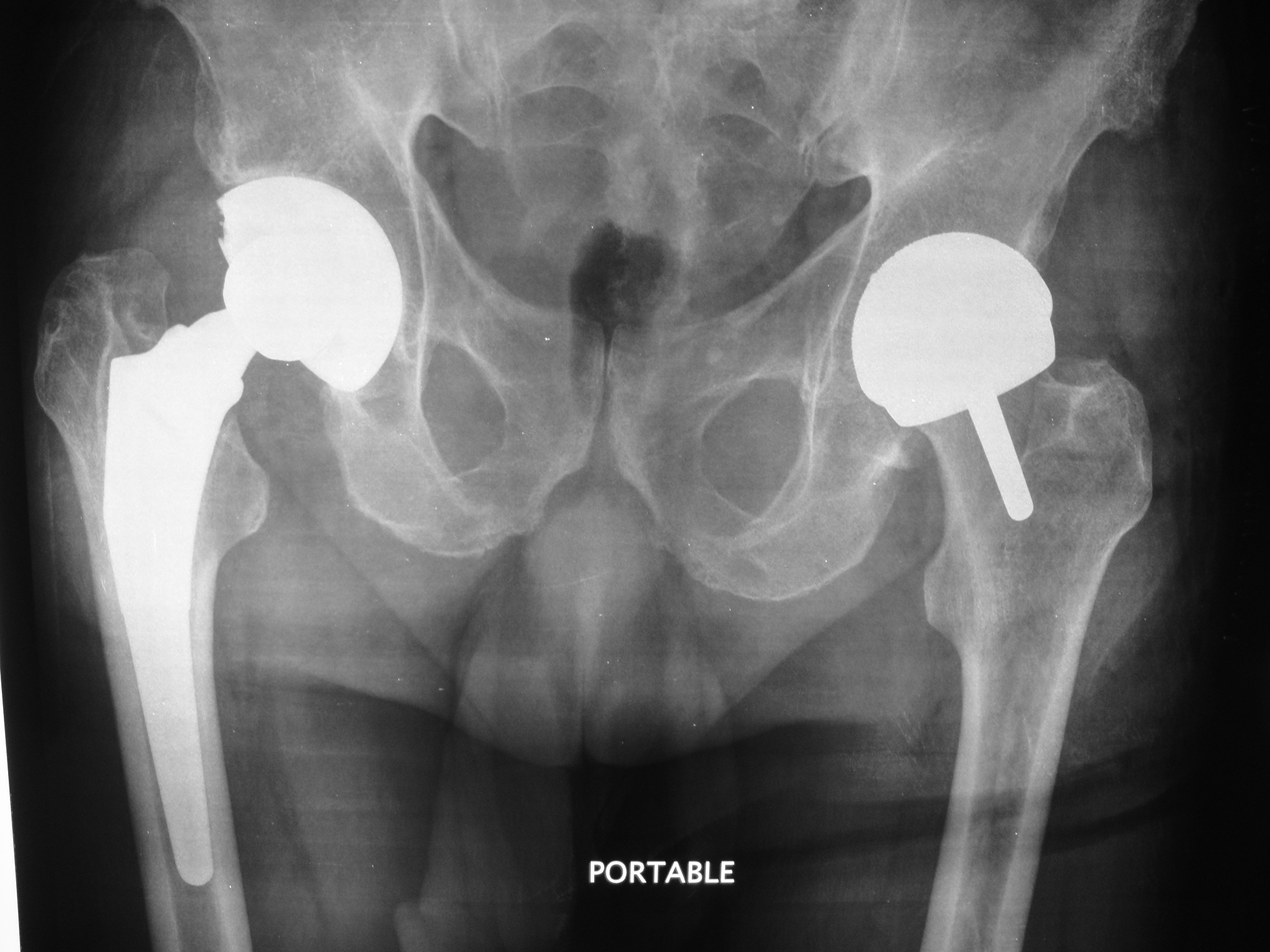
(Image from the Cleveland Clinic.)
There are several purported advantages to resurfacing over replacement, the biggest being activity level. While most surgeons discourage running and other high-impact activities after a total hip replacement, there are generally far fewer long-term restrictions after resurfacing. After approximately one year post surgery, many resurfacing patients are allowed to run, jump, and engage in other high-impact athletic activities. That’s partly because resurfacing typically recreates the natural size of your femoral head, which nearly eliminates the risk of dislocation.
Other purported advantages are that resurfacing preserves more bone, provides more natural biomechanics, feels more natural, may reduce the risk of thigh pain associated with the femoral stem in a total hip replacement, and can be converted to a total hip replacement if needed. The latter is one reason proponents recommend resurfacing for younger patients in particular: younger patients are more likely to outlive their artificial hip and require a revision. Proponents of resurfacing believe it is easier to convert a resurfacing to a total replacement than to revise a total replacement itself.
Online you can find lists of athletes who have had resurfacings. I don’t follow tennis, the NHL, MLB, or NBA, so I don’t recognize most of the names. However, I do know that wrestler James Green had a hip resurfaced in 2023 and just won the U.S. Open in 2026. Tour du France rider Flloyd Landis also had a hip resurfaced by James Pritchett and then returned to competitive cycling.
Andy Jones-Wilkins is an ultrarunner who had both hips resurfaced by Thomas Gross. He blogged about his surgeries and his successful return to ultrarunning. Ultimately, however, he had both hips revised, opting to replace his resurfacings with ceramic-on-ceramic total hip replacements. The revisions were successful as well, and he again returned to ultramarathons. In 2025, he completed the Cocodona 250. He shares his full story during this 2025 interview.
Here’s a different interview with Jones-Wilkins and two other trail runners, one of whom had a resurfacing and another who had a total replacement. The runner who had a resurfacing said that if her other hip needs replacing in the future, she will get a total replacement rather than resurfacing. The runner who had a total replacement said that she runs a little bit of trails every day.
Whatever the advantages, there are several concerns with hip resurfacings.
In Part II, we examine the criteria for patient selection, known risks like metal debris, and how long-term outcomes compare to total hip replacements.
According to the American Association of Orthopedic Surgeons, unlike hip replacement, hip resurfacing is not suitable for all patients. Generally speaking, the best candidates for hip resurfacing are younger than 60, have larger frames and strong, healthy bones. “Patients who are older, female, and smaller-framed, with weaker or damaged bone are at higher risk of complications, such as femoral neck fracture.”
In addition, according to Justin Cobb, a surgeon at the Cleveland Clinic in London, “Patients with smaller bones, including many women, are more likely to report pain after metal-on-metal hip resurfacing and require early revision. The pain is often due to soft tissue impingement on the oversized components or the tissue’s reaction to metal ion particles released with wear. These problems led to metal-on-metal resurfacings being withdrawn from use in women and smaller men in 2015.” In response, Cobb developed a ceramic-on-ceramic resurfacing implant, called H1, for patients with smaller hips and pelvises. H1 and other non-metal resurfacing options will be discussed in my next post, Replacement vs. Resurfacing (Part 2).
Because the stem inserts into the femoral neck, there’s a risk the neck can fracture, in which case the patient will probably need a total hip replacement. Resurfacing patients are typically screened based on bone density and size of their femoral head. To minimize the risk of fracture post-surgery, many resurfacing surgeons restrict their patients to crutches for the first four weeks or more. Additional restrictions last up to twelve months post-op.
A retrospective analysis of the resurfacings of Peter Brooks of the Cleveland Clinic states:
“We recommend a conservative postoperative return to activities, with six weeks of partial weightbearing using crutches, and avoidance of strenuous exertion, running and jumping for a full year.” Here are some more specific restrictions from Prem Ramkumar, lead author of the analysis above, and a resurfacing surgeon in Los Angeles:
Though a femoral neck fracture is impossible in a total hip replacement (because the femoral neck has been removed), the femur itself can fracture because of the inserted stem. In both cases, the risk of fracture tends to increase with age. However, several studies (admittedly from around 20 years ago) show a 1–2% risk of a neck fracture with resurfacing within the first year. In contrast, a 2024 UK study found the individual risk of a femoral fracture after THA to be 1% in 10 years, and a 2025 British study found the risk to be 0.6% in a median follow-up of 6.5 years.
For years, nearly all hip resurfacings have used metal-on-metal hardware. In fact, metal-on-metal constructs are the only resurfacing implants approved in the U.S.
The problem with metal-on-metal is that friction during normal use causes wear that sheds metal particles and ions into the hip joint. Those particles and ions can damage local tissue and bone, and the ions can enter the bloodstream, possibly causing damage to other organs.
Proponents of metal-on-metal resurfacings argue that debris-related problems were primarily limited to early designs with poor metallurgy or to improperly positioned implants, and that current designs, when properly positioned, do not cause adverse local tissue reactions (ALTR), metallosis, or elevated metal ion levels. (For a history of hip resurfacing, see this article.)
However, the 2025 Australian National Joint Replacement Registry reports that “metal related pathology” was the second most common reason for hip resurfacing revision (Table HT110), with the registry explicitly noting that the data presented are restricted to modern prostheses.
In addition, the 2025 UK National Joint Registry shows that metal-on-metal resurfacings have a 9.86% cumulative revision rate at 10 years — more than three times that of ceramic-on-polyethylene or metal-on-polyethylene total hip replacements (22nd Annual Report, 2025, Table 3.H5).
Patients with metal-on-metal joints are typically encouraged to have annual blood tests to check for elevated levels of cobalt and chromium — the two major components of most metal-on-metal bearings. According to a statement by the American Association of Orthopaedic Surgeons, a 2010 British safety alert set threshold levels for each at 7 ppb, recommending imaging studies when that value is exceeded. However, a 2011 study found that a lower threshold of 5 ppb was optimal, increasing sensitivity of the test from 52% to 64%.
A 2013 study using MRI found that 31% of asymptomatic metal-on-metal resurfacing patients had ALTR. It also reported that 92% of asymptomatic patients with ALTR had chromium levels below the 7-ppb threshold, and 85% had cobalt levels below the same threshold. The article also notes that previous studies reported ALTR rates of 5%, 30%, 61%, and 68% in asymptomatic resurfacing patients.
Similarly, a 2021 study at HSS using MRI found that 25% of hip resurfacing patients had ALTR. Patients with MoM resurfacings had higher cobalt and chromium serum ion levels than those with CoP total hip replacements, and they were nearly 5 times as likely to have ALTR or metallosis compared. Many patients with ALTR were asymptomatic and did not have levels of metal ions in their blood exceeding the thresholds.
The lead author stated:
We found that patients can be completely asymptomatic and have high-functioning hip scores while harboring reactions that could start to destroy the soft tissues around the hip. (Source)
These data underscore that adverse local tissue reactions can occur in high functioning, asymptomatic individuals with good function scores and that serum ion levels and symptoms alone are not predictive of the presence and magnitude of adverse local tissue reactions. (Source)
A press report from HSS concludes:
...the use of MRI should be included as part of routine follow-up protocol for hip replacement patients, as an annual clinical assessment dependent on survey or blood metal ion testing alone may not detect complications.
Finally, a 2013 study at HSS found synovitis in 68% of asymptomatic hips with metal-on-metal resurfacings.
Even some surgeons who perform resurfacings advise against them. Presley Swann (a surgeon in Denver) says that he performs resurfacings, but only for patients who request it and understand and accept the risks. He says he would not have one himself. Instead, he would opt for a traditional total replacement. His main concern is metal debris, which he says can trigger an immune response that destroys soft tissue beyond repair.
There are far fewer hip resurfacings performed each year than total replacements.
The 2025 Annual Report of the American Joint Replacement Registry recorded over 1.4 million total hip replacements versus less than 7,000 resurfacings between 2012 and 2024. (99.5% vs. 0.5%). In 2024 alone, the registry captured just shy of 160,000 replacements versus just 44 resurfacings. (99.7% vs. 0.3%)
Similarly, in Australia, resurfacings represented just 2.9% of hip replacements from 1999 to 2024, and just 1.1% of hip replacements in 2024. (2025 Annual Report, Table HT1; 2025 Lay Summary.)
In the UK, resurfacings have declined from 10% of all hip arthroplasties in 2004 to less than 1% every year from 2015 to 2024 — with just 0.6% in 2024. (2025 Annual Report, Table 3.H2)
No surgeon I talked with at UCLA, USC, Cedars-Sinai, or Torrance Memorial recommended hip resurfacing. All expressed concern about metal-on-metal wear and debris. One of the surgeons performed resurfacings in the past, but stopped. Others had second-hand experience through colleagues, residencies, or fellowships.
James Pritchett lists other “drawbacks” that discourage surgeons from performing resurfacings: Resurfacing is a technically more difficult surgery that takes about 33% longer than a total replacement, yet U.S. insurance companies pay providers the same rate as for a total replacement. Resurfacing implants are more expensive and less available. Resurfacing tends to consume more staff and surgeon time because of the self-selected population: they are more active, more concerned about what’s possible post-surgery, and thus ask more questions. (The interview time for resurfacing patients averages 49 minutes, compared with 24 minutes for total hip replacement patients.) Finally, Pritchett says the patient has to be the right candidate: they have to have an athletic need for a resurfaced hip, and anticipate 20 years of athletic use. Otherwise, he says, a total hip replacement is an excellent option.
Regardless of the reasons, the fact remains that resurfacing is a niche procedure performed by a small number of surgeons. Even advocates of resurfacing acknowledge: “Given the relative rarity of this procedure in the USA, it is likely that few surgeons currently have both the experience and the comfort level to perform hip resurfacing with proficiency.”
The website “SurfaceHippy” maintains a list of surgeons who have performed more than 1,000 resurfacings. There are just 12 in the U.S. and just 14 more in other countries. James Pritchett and Thomas Gross seem to be the volume leaders in the U.S., with Pritchett having performed over 10,000 resurfacings and Gross over 7,000. Surgeons at prestigious institutions in the U.S. who perform hip resurfacings include Edwin Su at the Hospital for Special Surgery in New York City, Peter Brooks at the Cleveland Clinic in Florida, Scott Marwin at NYU, and Robert Barrack at Washington University in St. Louis.
In Part 2, I’ll review studies comparing the outcomes of resurfacing vs. replacement and will explain why I decided to have a total replacement.
- - -
Posted June 2026.